Did you know there is a government “grant” given to some of the most privileged in the country? Those who have the resources to be able to afford private medical aid get R364 deducted from their tax every month. While it might be disguised under the name of a “tax credit”, the effect is the same – the state is giving them money. This costs the state R30 billion every year.
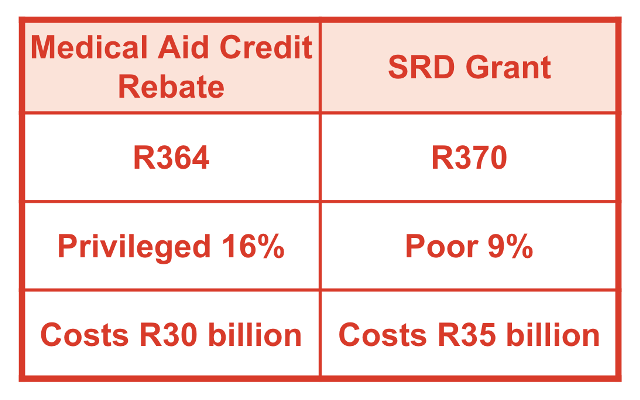 Contrast this with another grant, the Social Relief of Distress (SRD) grant. This is a grant of R370 per month, available only to some of the poorest South Africans. The grant has only increased once since it was introduced, and its future still remains uncertain. Treasury claims that funding the grant is not sustainable. The grant costs the state R35 billion every year.
Contrast this with another grant, the Social Relief of Distress (SRD) grant. This is a grant of R370 per month, available only to some of the poorest South Africans. The grant has only increased once since it was introduced, and its future still remains uncertain. Treasury claims that funding the grant is not sustainable. The grant costs the state R35 billion every year.
Looking at these two grants side by side, the kind of economic theory and the politics of the Treasury become clear. They are happy to put money into the pockets of wealthier people, as they will “do productive things” with this money that will create growth. That growth will somehow trickle down to the rest. In addition, they say that they believe that incentivising people to use private services “to lessen the burden on the state” is worth paying for. It should be noted that all the people who make these decisions have medical aid and therefore benefit from this gift. None of them receives the SRD grant.
Now, there is no universal truth here; economic theory is inherently political. As with anything political, we must ask, who does this politics serve? There is plenty of evidence that trickle-down economics does not work. In this particular case, rather than spending this money, individuals with medical aid are much more likely to save or invest in financial assets that do little for growth. SRD recipients, on the other hand, are likely to spend, creating demand for goods and services, which in turn leads to growth. In fact, trickle-down economics is just a convenient narrative for why money is “best-off” in the hands of the elite.
Incentivising people to use private health care “to lessen the burden on the state” creates a two-tiered system: those in luck can access higher quality care. It also drains essential resources from the state. Far from taking a burden off the state, as some argue, its services are rendered using staff that the public sector needs and the state has trained. And it distances wealthier citizens, who hold significant political power, from public institutions, causing them to become detached from public health considerations. If those with money and power were still invested in the state of our public health, it would not have been allowed to deteriorate to the sorry state it is in today.
Some of the privileged 16% medical aid members are not ‘wealthy’ — they are middle class. While such a change will worsen their cost-of-living problems, this alone cannot justify providing what is essentially a form of government grant on the basis of medical aid membership. While the cost-of-living problems experienced by the middle and working class must be taken seriously, the medical aid credit rebate is a poorly targeted measure. It eases the cost of living for the middle class alone.
For more information on this and a host of other possible progressive tax reforms, see the Alternative Information and Development Centre’s new publication, Tax in the World’s Most Unequal Country: The South African Fair Tax Monitor on opportunities for resource mobilisation.
Chloé van Biljon is a Tax Justice Officer at the Alternative Information and Development Centre (AIDC).